Table Of Content
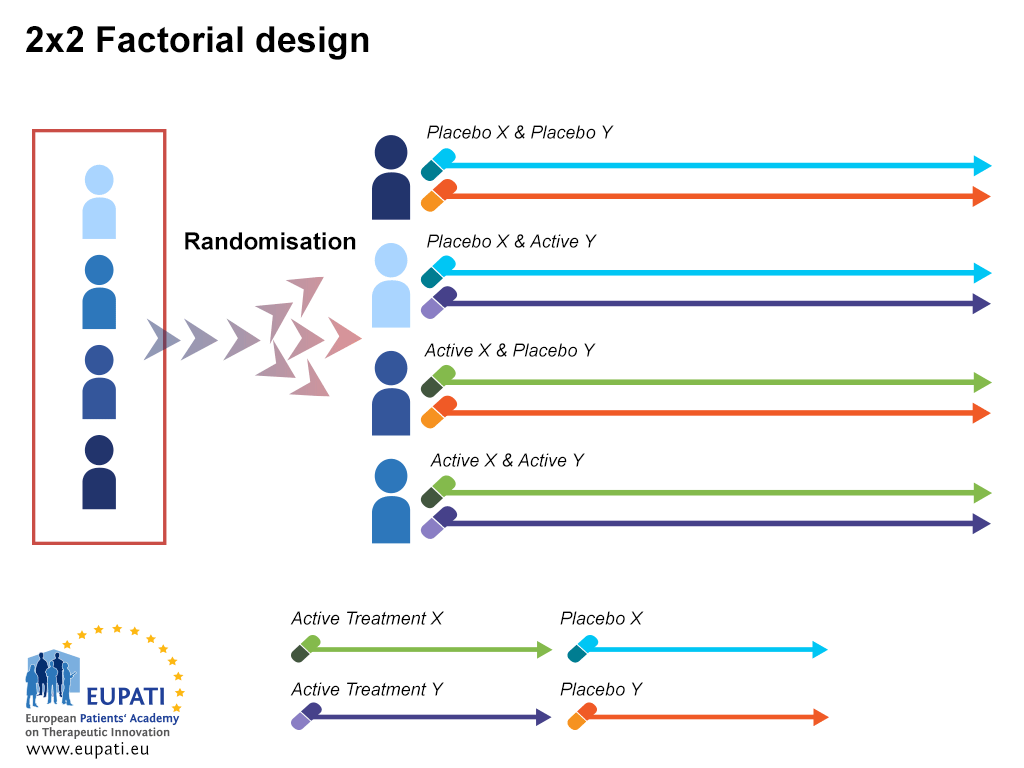
Below, we created a framework based on the risk that the trial will fail vs. the chance that results will be beneficial to help the investigator choose the appropriate phase design. This week, we explore different types of trial designs, including parallel, crossover, group allocation, factorial, large simple, equivalency, non-inferiority, and adaptive designs. (i) Switch back design (ABA vs BAB arms) – Drug A → Drug B → Drug A in one arm versus Drug B → Drug A → Drug B in other arm. The switch back and multiple switchback designs are of emerging relevance with the advent of biosimilars where switchability and interchangeability of a biosimilar to a bio-originator molecule can only be confirmed by such trial designs.
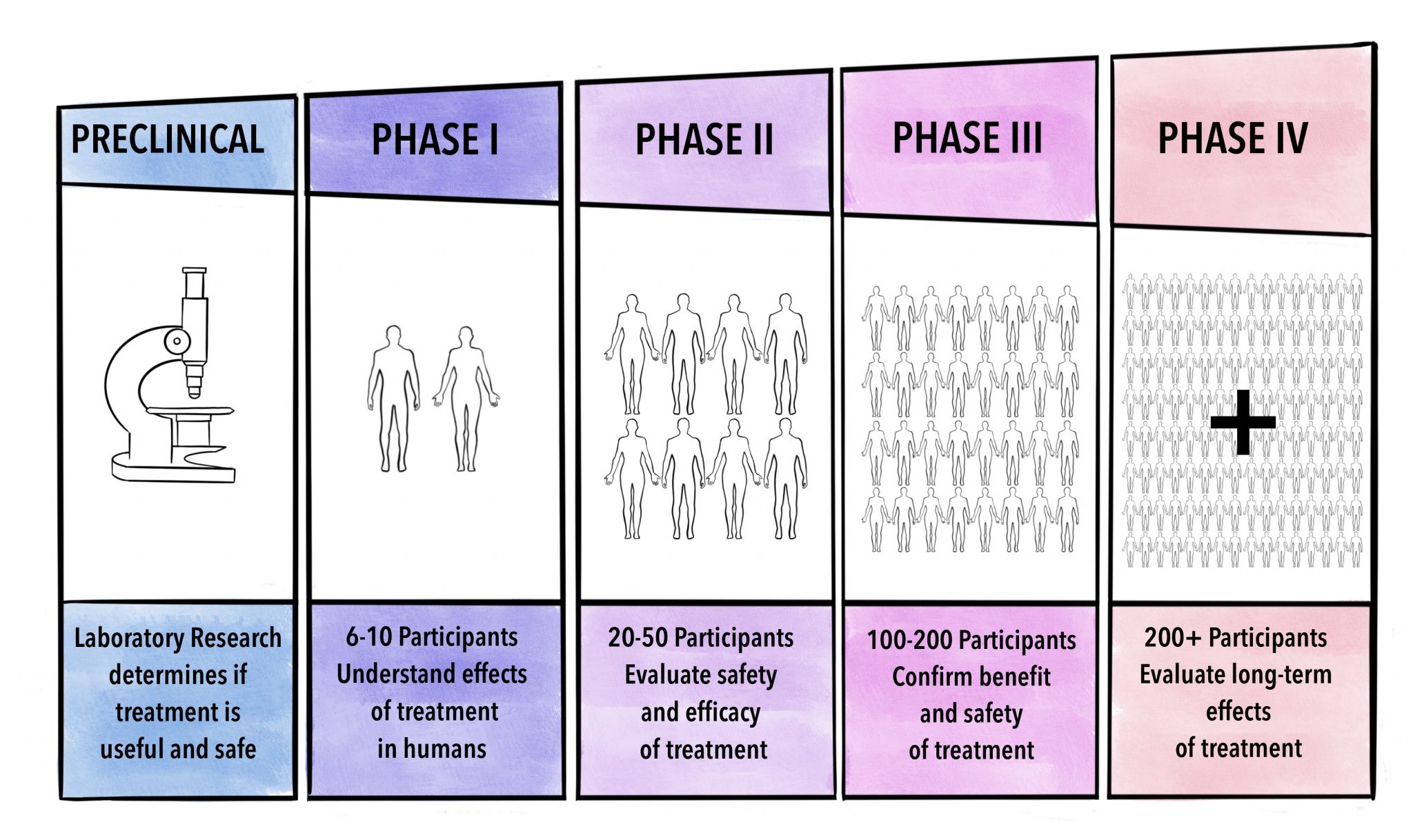
Clinical trial phases: pharmacological studies
Progressive trial phases require higher levels of evidence and sophistication, depending on the preliminary data and research question. While conducting trials in progressive phases increases trial challenges and short-term costs, this method is important to enhance safety and decrease long-term costs. In fact, late trials (e.g. phase III trials), which have a large number of subjects and are more costly, must have a strong signal from early less costly clinical trials in order to enhance chances of success. The course will explain the basic principles for design of randomized clinical trials and how they should be reported.
Clinical trial design during and beyond the pandemic: the I-SPY COVID trial
When both potential benefits and risks are high, we recommend running pilot, phase I, or small mechanistic phase II studies to better evaluate and quantify the risks. But researchers need to be careful as investigations in this category can fail more often than in less risky trials. One example is a phase III trial investigating tDCS for neuropathic pain that was not based on strong preliminary data. Indeed, this trial failed and thus patients were unnecessarily exposed to risk (47).
Clinical trial phases: medical device studies
Most drugs studied (about 90%) never make it to market, as human trials do not show efficacy (27–29). Attrition is highly costly and frustrating, yet such studies help by showing us what does not work – “validation using known failures” (32) – assuming they are published. Clinical trials investigate new therapeutic interventions in a controlled environment, aiming to minimize biases and build on truth (1). Although experimentation has marked progress throughout human history, James Lind’s “A treatise of the scurvy” published in 1753 pioneered the methodology of modern controlled trials (1,2). Further progress on statistical and other methodological techniques (such as better blinding methods) together with improved ethical guidelines helped advance the science of clinical trial methodology.
Clinical trialists often use the terms “single-blind” to indicate blinding of study participants, “double-blind” to indicate blinding of study participants and investigators, and “triple-blind” to indicate blinding of participants, investigators, and the sponsor and assessors. Community trials are also known as cluster‐randomized trials, involve groups of individuals with and without disease who are assigned to different intervention/experiment groups. One-year efficacy results for the first patient in cohort 2 showed a positive clinical evolution, with a clear inflection of clinical score North Star Ambulatory Assessment (NSAA). Other functions assessed (10 Meter Walk Test and ability to stand up) also showed a positive trend. About HB-200HB-200 is HOOKIPA’s lead oncology candidate engineered with the company’s proprietary replicating arenaviral vector platform.
It is important to actively anticipate major challenges and ways to deal with them while still in the design phase. The impact of improving medical knowledge is conditional on this knowledge changing clinical practice. Thus, surrogate outcomes should not stand alone but be clinically validated, and clinical outcomes should reach the minimum clinically important difference. Eventually, study outcomes should lead to cures and treatments for previously untreatable conditions, improved therapeutic options for different patient subgroups, more efficient or less costly healthcare delivery, or similarly meaningful improvements to healthcare. Randomization should balance known and unknown factors between intervention groups (41), such that different results can be causally attributed to the intervention rather than to confounders. To maintain this balance, all randomized subjects should be analyzed (intention-to-treat analysis).
They retrospectively reviewed a defined cohort for cases with and without neonatal tetanus.9 They found a strong association of the application of ghee (clarified butter) as a risk factor for neonatal tetanus. Although this suggests a causal relationship, cause cannot be proven by this methodology (Figure 3). The purpose of sample size calculation is to determine the number of patients needed to enroll in the study to provide sufficient information to address the primary objectives.
Repurposing a diabetes drug to treat Parkinson’s disease
Subsequently the non-PASI 75 achievers are dropped from the trial due to lack of efficacy. PASI 75 responders are continued on the drug or are assigned to placebo and retention of PASI 75 response at 1 year after randomization can be compared between two arms. If there is no statistically significant difference in outcomes between the arms, an expensive biological can be administered till PASI 75 is achieved and then omitted, thereby reducing cost of therapy. Illustrative example – A comparative trial of Acitretin and Apremilast in palmoplantar psoriasis, where there exits clinical equipoise as regarding efficacy can be conducted as a randomized controlled (acitretin as active control) parallel arm trial design. This design is usually utilized to determine pharmacokinetic properties of a new drug (Phase 1 trials). Uncontrolled trials are known to produce greater mean effect estimates than a controlled trial, thereby inflating the expectations from the intervention.
Accelerating stakeholder collaboration to enhance the clinical trials environment in the EU European Medicines Agency - European Medicines Agency
Accelerating stakeholder collaboration to enhance the clinical trials environment in the EU European Medicines Agency.
Posted: Wed, 20 Mar 2024 07:00:00 GMT [source]
Thus, it is important that to maximize the chances that the trial will be Feasible, Interesting, Novel, Ethical and especially Relevant (FINER criteria). The mission of The Johns Hopkins University is to educate its students and cultivate their capacity for life-long learning, to foster independent and original research, and to bring the benefits of discovery to the world. This week, we focus on whether RCTs are still the gold standard for evaluating evidence.
Significant progress has been made in kidney transplantation, with one-year graft survival nearing 95% [1]. However, long-term allograft survival remains suboptimal, with a 10-year overall graft survival rate of only 53.6% for deceased donor transplant recipients [2]. This review aims to discuss opportunities for improving retrospective and prospective studies of ABMR, focusing on addressing heterogeneity, outcome measurement, and strategies to enhance patient enrollment to inform study design, data collection, and reporting. Early phases of clinical studies include pilot studies, phase I, phase II single arm, and proof of concept. Later phases of clinical studies include randomized phase II, phase II/III, and phase III trials.
In this article, we present some general design principles for investigators and their research teams to consider when planning to conduct a trial. Safety is defined by how much an intervention increases patients’ risks of having adverse events (especially serious ones such as death or hospitalization). A solid understanding of the literature and putative mechanisms of action leads to an enhanced appraisal of the intervention’s safety and probable future adverse events. Lacking mechanistic data leads to an increased risk of unexpected results even if the trial design eliminated all or most sources of bias. In fact, a limited understanding of the disease process is often highlighted by an abundance of negative trials, e.g. in PLP.
Therefore modern medicine has seen great advances as trial design and quality improved over the past 60 years, leading to better internal validity, efficiency and reporting (3). In this design, subjects are randomized to one or more study arms and each study arm will be allocated a different intervention. After randomization each participant will stay in their assigned treatment arm for the duration of the study [Figure 5].
Note however that the fact that trial participants in neither intervention arm adhere to therapy may indicate that the two interventions do not differ with respect to the strategy of applying the intervention (i.e., making a decision to treat a patient). Researchers need to be careful about influencing participant adherence since the goal of the trial may be to evaluate the strategy of how the interventions will work in practice (which may not include incentives to motivate patients similar to that used in the trial). The selection of a population can depend on the trial phase since different phases have different objectives. Early phase trials tend to select populations that are more homogenous since it is easier to reduce response variation and thus isolate effects. Later phase trials tend to target more heterogeneous populations since it is desirable to have the results of such trials to be generalizable to the population in which the intervention will be utilized in practice.
Ideally endpoints could be measured objectively (e.g., via a laboratory test) however many endpoints are based on subjective evaluation. Variation in these diagnoses can be minimized with clear definitions and consistent evaluations. Issues in trial conduct and analyses should be anticipated during trial design and thoughtfully addressed. After eliminating or significantly decreasing potential biases, the investigator still needs to design a strong trial with a high likelihood of confirming the main hypothesis. The strength of a trial will be based on the previous clinical and mechanistic evidence supporting its design.
Furthermore, Bolognini et al. evaluated the effects of 5-day transcranial direct current stimulation (tDCS) on the motor cortex of 8 amputees with PLP, based on the theory of maladaptive plasticity (10). These trials found promising effects of neuromodulation to alleviate PLP (low risk approach with high potential benefits). Other pilot studies concerned the application of sympathetic blocks (24) and cryoablation (12) for the treatment of PLP.
This atypical presentation is usually described as case reports which provides a detailed and comprehensive description of the case.4 It is one of the earliest forms of research and provides an opportunity for the investigator to describe the observations that make a case unique. There are no inferences obtained and therefore cannot be generalized to the population which is a limitation. Most often than not, a series of case reports make a case series which is an atypical presentation found in a group of patients. This in turn poses the question for a new disease entity and further queries the investigator to look into mechanistic investigative opportunities to further explore.








No comments:
Post a Comment